Intravenous (IV) liothyronine is used to treat severe hypothyroidism resulting in myxoedema and myxoedematous coma. But Graves’ disease, which causes hyperthyroidism, is also associated with myxoedema in the form of infiltrative dermopathy or pretibial myxoedema. Can liothyronine be used to treat pretibial myxoedema? But, if we give IV liothyronine to someone with Graves’ disease suffering from pretibial myxedema, wouldn’t this cause thyroid storm instead?
Myxoedema refers to a relatively hard oedema (as opposed to a soft, fluid oedema) caused by the accumulation of mucopolysaccharides in the interstitial fluids.
The term “myxoedema” alone refers to generalised myxoedema and is used to describe severe hypothyroidism characterised by myxoedema of cutaneous tissue together with other symptoms including somnolence, slow mentation, dryness and loss of hair, ascites, hypothermia etc. This is a severe condition that can result in coma and death. The accumulation of mucopolysaccharides is a direct result of the hypothyroidism as thyroxines are required for their turnover.
When IV liothyronine is used for the treatment of myxoedema or myxoedematous coma, it is the treatment of this form of severe hypothyroidism that is being referred to.
“Pretibial myxoedema” refers explicitly to infiltrative dermopathy localised in the pretibial area (the shin). In this case, the infiltration and accumulation of mucopolysaccharides (especially the glycosaminoglycan hyaluronic acid) is due to secretion from fibroblasts. The pathogenesis is not caused by thyroid hormone levels. The exact pathogenic mechanism is not known, but it is generally thought that it is due to the autoimmune response. Fibroblasts express TSH receptor protein and are likely targeted by the TSH receptor antibodies produces in Graves disease. Cytokines secreted by Th1 type T cells activated by TSH receptor antigen may also stimulate fibroblasts to secrete glycosaminoglycans.
Pretibial myxoedema is not treated with IV liothyronine as thyroid hormone levels are not responsible for this localised inflammatory myxoedema.
Reference:
Davies, TF. Pretibial myxedema (thyroid dermopathy) in autoimmune thyroid disease. Ross, DS, Mudler, JE ed. UpToDate. Waltham, MA: UpToDate Inc. http://www.uptodate.com (Accessed on January 8, 2018).

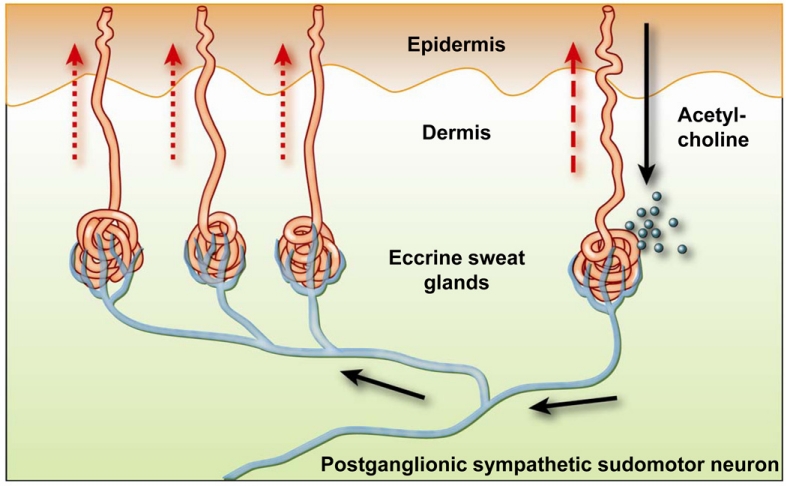 Image credit:
Image credit: